
As of late January 2026, the emergence of the Nipah virus in West Bengal has triggered a predictable global reflex. From thermal scanners at Bangkok’s Suvarnabhumi Airport to heightened vigilance in Singapore, the international community is on edge. However, an analysis of the data from the National Centre for Disease Control (NCDC) reveals a localized event successfully ring-fenced by public health protocols.
Fact Box
| Category | Confirmed Reality | Speculative Rumors |
| Confirmed Cases | 2 laboratory-confirmed cases | Reports of “nationwide” spread |
| Patient Profile | 2 Healthcare Workers (Nurses) | Widespread community infection |
| Location | Barasat, West Bengal | Conflation with 2025 Kerala cases |
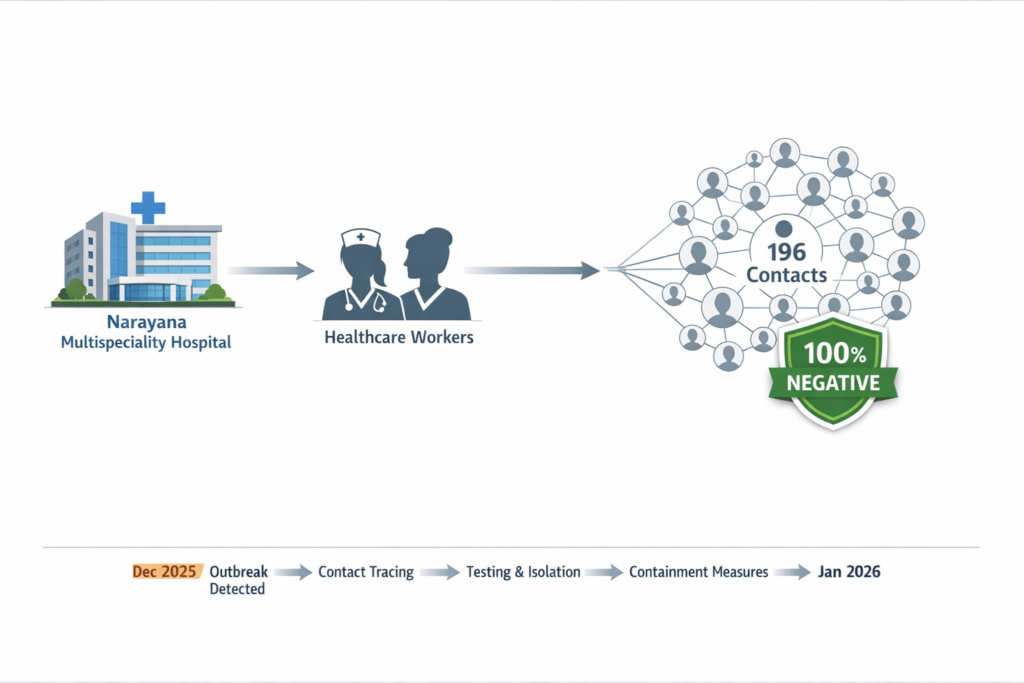
| Contact Status | 196 identified; 100% negative/asymptomatic | Undisclosed secondary clusters |
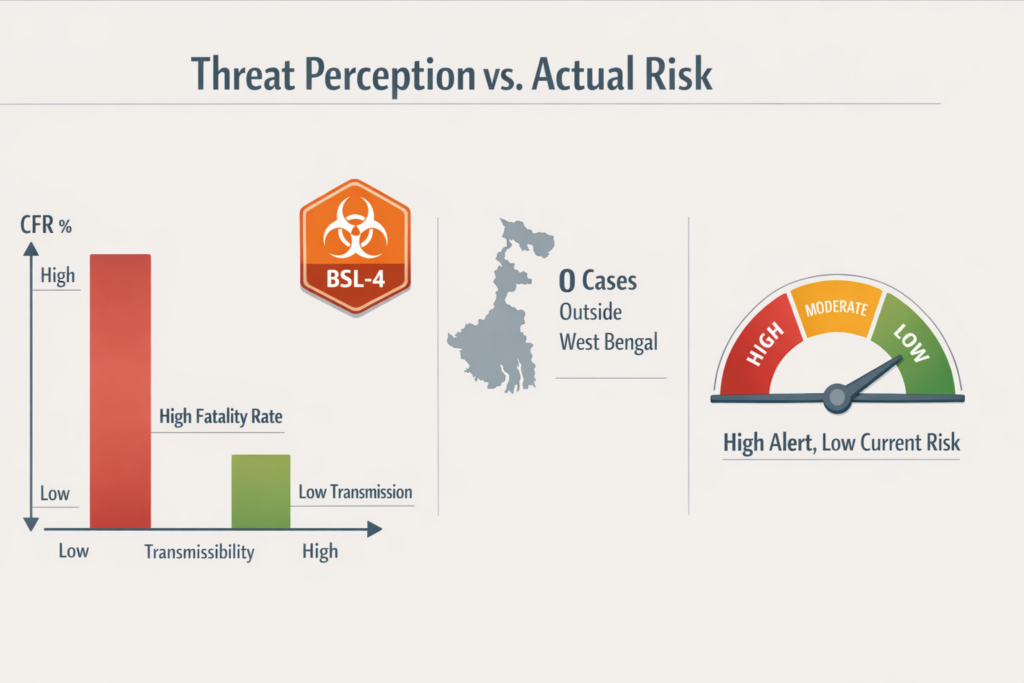
| Global Detection | 0 cases detected outside West Bengal | Cross-border “runaway” transmission |
Addressing the Panic
The current atmosphere surrounding the Nipah virus is defined by a gap between border-screening headlines and clinical reality. In Thailand and Nepal, travelers from India are met with thermal scanners and “Beware” cards, creating the impression of an impending plague. This response reflects the high stakes of a pathogen with a 40% to 75% fatality rate and no available vaccine.
However, the situation on the ground in Kolkata is one of “Controlled Containment.” According to the official NCDC Clarification issued on January 27, 2026, there is no evidence of a nationwide spread. The event is restricted to a single hospital-linked cluster. While international hubs react to the possibility of transmission, Indian health authorities have already effectively broken the chain, as confirmed by the negative test results of all 196 primary contacts.
The Outbreak Specifics
The 2026 event originated at the Narayana Multispeciality Hospital in Barasat, North 24 Parganas. The two confirmed cases involve a male and a female nurse who were on duty together in late December 2025. Epidemiological investigations suggest a Zoonotic Spillover that underwent nosocomial (hospital-based) amplification. The nurses were likely exposed while treating an “index patient” who presented with severe respiratory distress and died before Nipah testing could be initiated.
By January 4, both West Bengal Healthcare Workers developed high fever and respiratory distress, progressing toward encephalitis. They were immediately isolated in specialized infectious disease facilities. Diagnostic confirmation was provided by AIIMS Kalyani and the National Institute of Virology (NIV) in Pune using RT-PCR, identifying the NiV-Bangladesh clade. This clade is known for human-to-human transmission potential, yet the swift activation of isolation protocols prevented further spread within the facility or the community. Unlike the 2025 Kerala outbreaks, which involved community spillover, this was a contained medical breach.
“Category 5” Precautions
The Kolkata Airport Screening measures in neighboring nations are often misinterpreted as evidence of an escalating crisis. In reality, these are precautionary biosafety protocols. Thailand has screened over 1,700 passengers from West Bengal without detecting a single positive case. Nepal has established health desks at the Kathmandu airport and land border crossings in Koshi Province to monitor trans-border movement.
In Taiwan, the CDC has proposed listing Nipah as a “Category 5” notifiable disease. This is a legal classification for rare emerging infections that mandates immediate reporting and allows for government intervention; it is not an indicator that the virus has reached Taiwan. Similarly, Singapore’s Communicable Diseases Agency (CDA) has implemented temperature checks for flights from affected areas. These actions are defined by the “Science of Panic”: when a virus has a high fatality rate and no licensed treatment, the margin for error is zero. These measures are designed to maintain a “zero-case” threshold rather than manage an active outbreak.
The Science of Panic: Why the Reaction is Extreme
The global anxiety stems from Nipah’s biological profile, not its current prevalence. It is classified as a Biosafety Level 4 (BSL-4) pathogen with pandemic potential. The combination of a high Case Fatality Rate (CFR)—historically reaching 100% in some Indian clusters—and the lack of an approved vaccine makes every case a global security concern.
Furthermore, the NiV-Bangladesh strain involved in this cluster has a documented history of spreading among close contacts and healthcare providers. However, it is essential to distinguish between lethality and transmissibility. Nipah typically requires direct contact with infected bodily fluids and does not spread easily through casual contact. The risk to the general public outside the Barasat medical cohort remains essentially nil.
A Calm Assessment of the “All Clear”
The 2026 West Bengal situation is a case study in successful intervention overshadowed by digital alarmism. The definitive metric of this event is the “All Clear” signal regarding the 196 traced contacts. When 100% of high-risk individuals—including family members and other medical staff—test negative after the 21-day incubation window, the outbreak can be considered broken.
For the public, the message is one of vigilance, not fear. The airport scanners are necessary safeguards, but the domestic reality in India is one of effective containment. By relying on verified reports from the NCDC and the WHO, we can navigate this situation with precision. The West Bengal cluster demonstrates that even the deadliest viruses can be managed through rapid detection and transparent reporting.
READ OUR OTHER ARTICLES
- Know the Real Reason Behind Tarun Kumar’s Death Over a Holi Balloon
 The Holi festival turned tragic in southwest Delhi this year. On Wednesday, March 4, 2026, the narrow lanes of a JJ Colony in Uttam Nagar became the center of a … Read more
The Holi festival turned tragic in southwest Delhi this year. On Wednesday, March 4, 2026, the narrow lanes of a JJ Colony in Uttam Nagar became the center of a … Read more - T20 World Cup Final 2026: India vs New Zealand
 The cricket world is getting ready for its biggest event. On Sunday, March 8, 2026, the T20 World Cup 2026 final will take place. The stage is set for a … Read more
The cricket world is getting ready for its biggest event. On Sunday, March 8, 2026, the T20 World Cup 2026 final will take place. The stage is set for a … Read more - 1,000-Year-Old Kakatiya Vishnu Idol Found in Telangana
 The quiet forests of the Jayashankar Bhupalpally district in Telangana recently gave up a secret they had been keeping for a thousand years. In March 2026, as the summer heat … Read more
The quiet forests of the Jayashankar Bhupalpally district in Telangana recently gave up a secret they had been keeping for a thousand years. In March 2026, as the summer heat … Read more - Kerala Set to Manufacture BrahMos Missile on 180-Acre
 India’s plan to become self-reliant in defense took a major leap forward on March 2, 2026. On this day, the Kerala Cabinet made a historic decision to give 180 acres … Read more
India’s plan to become self-reliant in defense took a major leap forward on March 2, 2026. On this day, the Kerala Cabinet made a historic decision to give 180 acres … Read more - Why Aman Gupta Chose His Birthday to Reveal OFF/BEAT ?
 On March 3, 2026, the Indian startup world saw a digital shift that was as much about legacy as it was about the future. Aman Gupta, the famous co-founder of … Read more
On March 3, 2026, the Indian startup world saw a digital shift that was as much about legacy as it was about the future. Aman Gupta, the famous co-founder of … Read more